








1. INTRODUCTION
- The process of separation and elimination of metabolic wastes, excess water and salts from cell tissues, organs and the body to the outside is known as excretion. These metabolic wastes accumulate in the body, if they are not removed from time to time and produce toxic effects. Basically the metabolic wastes are of two types i. A nitrogenous and non-nitrogenous.
- Both excretion and osmoregulation are required for the maintenance of homeostasis.
- Kidneys are involved in the homeostasis of the body fluids and also maintain acid-base balance by excreting H ions
- Dehydration kills a person much faster than lack of food. Water is the most important constituent of protoplasm, the living substance.
2. MODES OF EXCRETION
- Ammonia, urea and uric acid are the major forms of nitrogenous wastes excreted by the animals.
- Ammonia is the most toxic and requires large amount of water for its elimination, where as uric acid is the least toxic and can be removed with a minimum loss of water.
- No energy is spent for the production of ammonia where as the production of uric acid involves expenditure of more energy.
- Uric acid is produced by sauropsids, insects and mammals too by purine metabolism.
- Many mammals except apes, man etc., produce the enzyme ‘uricase’ by which they can convert uric acid into a more soluble ‘allantoin’.
- Some animals excrete amino acids and are known as aminotelic. Eg: Star fish and Holothuria
- Urea is 1,00,000 times less toxic than ammonia.
- The metabolism of excess amino acids, and the nitrogen bases of nucleic acids namely purines and pyramidines produce ammonia.
- Besides urea mammals produce uric acid also by purine metabolism.
- Cartilagenous fishes can store high concentration of urea to maintain isotonic medium with surrounding marine water.
- Cartilage fishes, many other salt water fishes and molluscs store large quantities of Trimethyl Amine Oxide (TMO) to protect their body proteins from damaging effect of urea.
- In ammonotelic animals, ammonia is generally excreted by diffusion across body surfaces or through gill surfaces, as it is readily soluble. Kidneys do not play any significant role in its removal. Eg: Protochordates, cyclostomes many bony fishes, aquatic amphibians and aquatic insects.
- Uricotelic animals excrete uric acid in the form of pellet or paste Ex: Reptiles, birds, land snails and
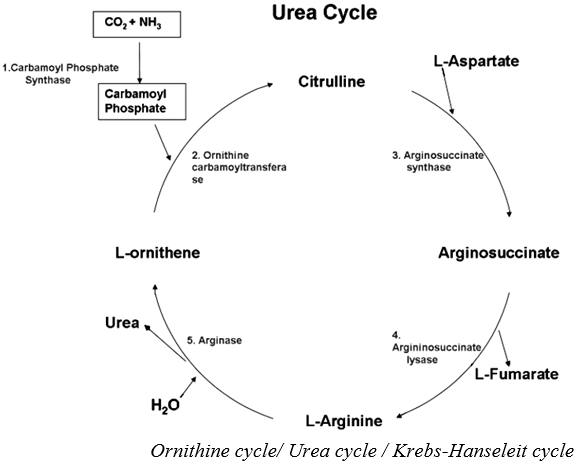
- insects.In ureotelic animals, ammonia produced by metabolism is converted into urea in the liver via the ornithine cycle, release into blood and excreted out by kidneys. Some amount of urea may be retained in the interstitial fluid of kidneys to maintain a desired osmolarity Eg: Mammals, terrestrial amphibians and cartilaginous fishes.
 3. EXCRETORY ORGANS
3. EXCRETORY ORGANS
- Protonephridia or flame cells are primarily concerned with osmoregulation. These are present in flat worms, rotifers, some annelids and Amphioxus (Cephalochordate).
- Nephridia in annelids and malpighian tubules in most of the insects, centipedes, millipedes help in the removal of nitrogenous wastes and osmoregulation.
Types of kidneys
- Pronephric kidney: Ciliated funnels or nephrostomes are present Eg., tadpole of frog and cyclostomes. It is also called anterior kidney.
- Mesonephric kidney: When Bowman’s capsule is present in uriniferous tubule, fish and frog, also known as mid kidney. Metanephric kidney: This is the most advanced kidney in which loop of Henle is present for each nephron. eg., reptiles, birds and mammals.
| Excretory organ | Function | Example |
| Protonephridia | Primarily associated with osmoregulaton and secondarily for excretion. | Platyhelminthes, rotifers some annelids, molluscan larvae |
| Protonephridia with solenocytes | Primary associated with osmoregulation and secondarily for excretion. | Cephalochordates |
| Metanephridia | Collect and eliminate waste materials from coelomic fluid. Perform osmoregulation too | Most annelids (Eg: Earthworm) |
| Malphigian tubules | Collect waste materials from haemolymph and release into hindgut. Help in osmoregulation also. | Insects, terrestrial arthropods. |
| Green (antennary) glands | Collect waste materials from the haemolymph and release exterior. | Exclusively crustaceans. |
| Coxal glands | Collect waste materials from the haemolymph and release exterior. | Arachnids |
| Pericardial glands | Collect waste materials from peri cardial fluid | Molluscs |
| Kidneys or metanephridia (or) Renal organs | Homeostasis in addition to excretion. | Molluscs and vertebrates. |
4. HUMAN EXCRETORY SYSTEM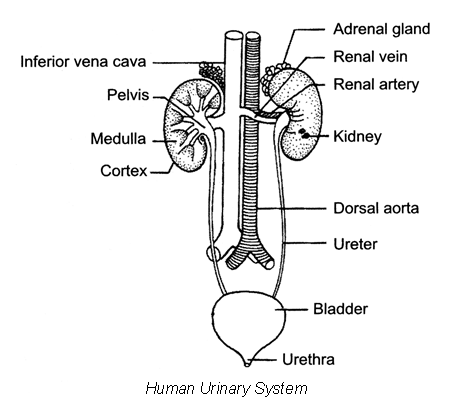
- Excretory system of humans consists of a pair of kidneys, a pair of ureters, urinary bladder and urethra.
- Kidneys are mesodermal in origin and are metanephric.
- Bean shaped, reddish brown kidneys with an average weight of 120-170g are situated between the levels of last thoracic and third lumbar vertebra close to the dorsal inner wall of abdominal cavity (retroperitoneal position).
- The right kidney is slightly lower than the left one due to the presence of liver.
- An artery enters and a vein along with an ureter exit the kidney through the hilum.
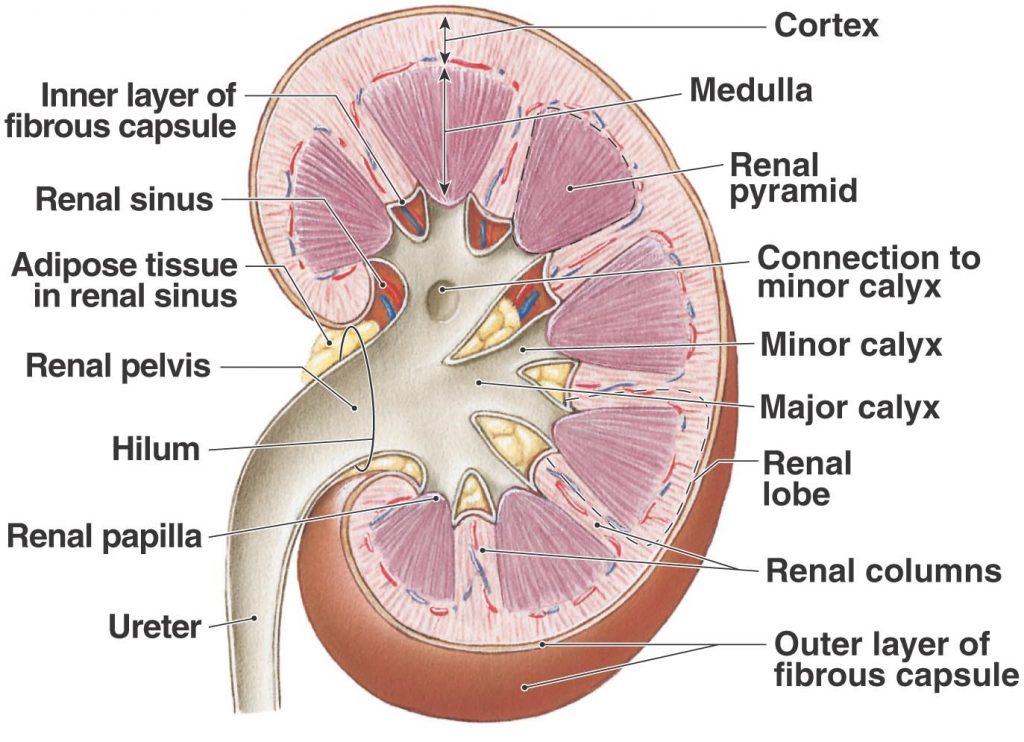
- Renal pelvis is a broad funnel shaped space inner to the hilum is with projections called calyces.
- Outer and inner zones in the kidney are called cortex and medulla respectively.
- Cortex extends in between the medullary pyramids as Columns of Bertini.
- Renal papillae project into cup like calyces, formed by the funnel shaped pelvis, which con-tinues out as the ureter.
- The walls of ureters are lined by transitional epithelium, they run downwards and open into the urinary bladder.
- Urinary bladder is also lined by transitional epithelium. The neck of the bladder leads into the urethra, which has an internal urethral sphincter(made of smooth muscles) and external urethral sphincter(made of striped muscles).
- Urethra opens near the vaginal orifice in the females and through penis in the
Structure of a nephron
- Each kidney has nearly one million functional units called nephrons.
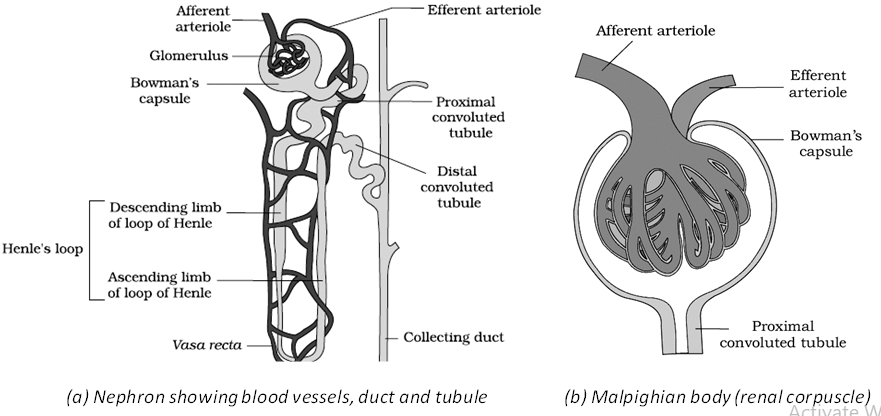
- Each nephron has glomerulus and the renal tubule.
- The renal tubule begins with a double walled cup-like structure called Bowman’s capsule, which encloses a tuft of capillaries formed by the afferent arteriole called glomerulus.
Longitudinal Section (Diagrammatic) of Kidney - Glomerulus along with Bowman’s capsule is called the malpighian body or renal corpuscle.
- Blood from the glomerulus is carried away by an efferent arteriole.
- The inner wall of the Bowman’s capsule is with the unique cells called podocytes, which leave intricate network of pores known as filtration slits or slit pores.
- The endothelial cells of the capillaries of glomorulus have pores or fenestrations.
- The tubule continues further as proximal convoluted tubule (PCT), Henle’s loop which has a descending and an ascending limb and distal convoluted tubule (DCT).
- Many DCTs open into collecting duct, many of which converge and open into the renal pelvis through medullary pyramids.
- The Malpighian corpuscle, PCT and DCT are in the cortical regions where as the loop of Henle dips into the medulla.
- The loop of Henle is too short in cortical nephrons and is very long in juxta medullary nephrons.
- Peritubular capillaries around the renal tubule and a ‘U’ shaped vasa recta runs parallel to the Henle’s loop they are formed from efferent arteriole.
- Vasa recta is absent or highly reduced in cortical nephrons.
 5. URINE FORMATION
5. URINE FORMATION 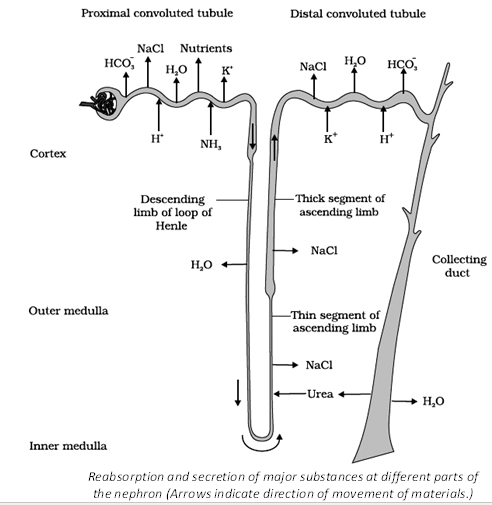 Glomerular filtration
Glomerular filtration
- The first step in urine formation is glomerular filtration. It occurs through 3 layers i.e the endothelium of glomerular blood vessels, the epithelium of Bowman’s capsule and a basement membrane between these two layers. This is a passive process.
- Net filtration pressure(NFP) causes the filtration and it is for about 10 mm Hg. NFP= Glomerular Hydrostatic Pressure – Glomerular Colloidal Osmotic Pressure + Capsular Hydro-static Pressure = (GHP – BCOP + CHP) = 60 – 32 + 18 = 10mm Hg
- The amount of the filtrate formed by the kidneys per minute is called glomerular filtration rate(GFR), it is approximately 125ml/minute i.e 180 litres/day.
- The filtrate is called glomerular filtrate or primary urine that contains almost all the constituents of plasma except proteins.
- About 85% of filtrate is reabsorbed in PCT and descending limb of loop of Henle in unregulated fashion. It is known as obligatory (or) mandatory reabsorption.
- Juxta glomerular apparatus is a special sensitive region formed by cellular modifications in DCT and the afferent arteriole at the location of their contact.
Selective Reabsorption and Tubular Secretion
- During tubular secretion, tubular cells secrete substances like H , K and ammonia into the filtrate, it helps in maintaining of ionic and acid base balance of body fluids.
- Based on the necessity of re-absorption, the substances of glomerular fliltrate can be categorized into high threshold substances-eg: glucose, amino acids,vitamins etc., low thershold substances- eg: urea, uric acid etc., athreshold substances-eg: Creatinine (actual waste material).
In the PCT
- PCT is lined by simple cuboidal brush border epithelium which increases the surface area for reabsorption.
- 70 – 80% of electrolytes, H2O , HCO3 and nearly all essential nutrients are reabsorbed, H , K and ammonia are selectively secreted into the filtrate in PCT(maintain the PH and ionic balance of the body fluids).
In the loop of Henle
- Henle’s loop plays a significant role in the maintenance of high osmolarity of medullary interstitial fluid.
- It’s descending limb is permeable to water but almost impermeable to electrolytes.
- Ascending limb is impermeable to water but allows transport of electrolytes actively or passively.
In the DCT
- Conditional reabsorption of Na, H2O
- takes place in DCT, it is also capable of reabsorption of HCO3 and selective secretion of H , K and NH3
- to maintain the PH and sodium-potassium balance in blood.
In the collecting duct
- Large amounts of H2O could be reabsorbed from collecting duct and it allows small amounts of urea into the medullary interstitium.
- Collecting duct plays an important role in the maintenance of pH and ionic balance of blood by the selective secretions of H and K ions.
- In the collecting duct the concentration of renal filtrate increases greatly and is now can be called urine (hypertonic).
- Conditional or facultative reabsorption occurs in DCT and collecting duct with the aid of ADH.
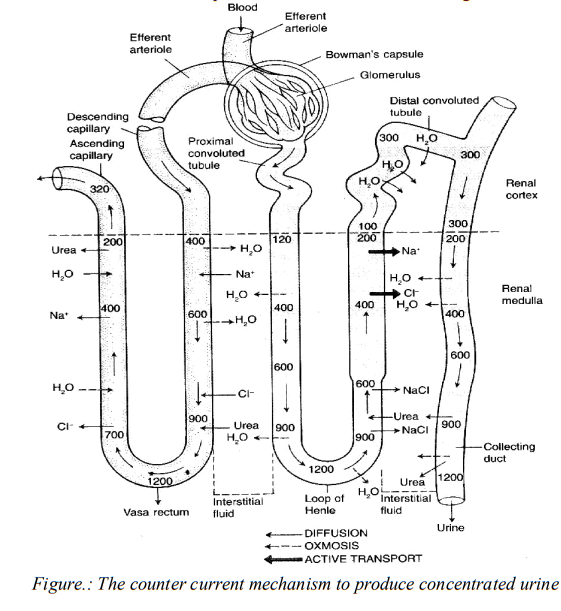
- In mammals the loop of Henle and the vasa recta have significant role in the formation of concentrated urine.
- The flow of renal filtrate in the two limbs of loop of Henle and the flow of blood in the two limbs of vasa recta are in opposite direction and thus forms counter current.
- From outer medulla to inner medulla the osmolarity increases 300 Osml/L to 1200 Osml/
- It is caused by NaCl and urea.
- NaCl reabsorbed from the ascending limb of loop of Henle and returns to the descending limb of vasa recta, hence osmolarity increases in the blood of vasa recta.
- NaCl from the ascending limb of vasa recta returns to medulla in exchange with water.
- Small amounts of urea enter the thin segment of ascending limb of loop of Henle and transports to medulla in collecting duct, thus osmolarity increases in medulla. To maintain balance, some
- water passes to the medulla and makes the filtrate hypertonic.
- Renal fluid in collecting duct becomes urine (4 times concentrated than initial filtrate).
6. OSMOREGULATION
- An excessive loss of fluid from the body can activate the osmoreceptors which stimulate the hypothalamus to release ADH or vasopressin from the neurohypophysis. It facilitates water reabsorption from later parts of the tubule.
- An increase in body fluid volume can switch off the osmoreceptors and suppress the ADH release to complete the feedback.
- ADH can also affect the kidney function by its constrictory effects on blood vessels.
- Defects in ADH receptors or inability to secrete ADH leads to diabetes insipidus resulting in dehydration and fall in BP.
7. REGULATION OF KIDNEY FUNCTION The functioning of kidney is efficiently regulated by hormonal feedback mechanism. It involves − Hypothalamus, Juxtaglomerular apparatus (JGA), and heart. HYPOTHALAMUS
- Antidiuretic hormone or ADH plays an important role in regulation.
- Excessive loss of fluids from the body activates the osmoreceptors and stimulates hypothalamus to release hormone ADH, which helps in water re-absorption and prevents diuresis.
- A further increase in body fluid volume can turn off the osmoreceptors. This inhibits the ADH release, which in turn completes the feedback.
- ADH constricts the blood vessels and causes blood pressure to increase, which in turn increases glomerular blood flow and therefore GFR.
JUXTAGLOMERULAR APPARATUS (RENIN-ANGIOTENSIN MECHANISM)
- When GFR falls, JG cells release renin.
- Renin plays an important role in the production of angiotensin II.
- Angiotensin II − Constricts blood vessels to increase blood pressure and hence GFR It also activates adrenal cortex to release aldosterone that causes re-absorption of Na+ and water from tubule. This also results in an increase in blood pressure and hence GFR.
HEART
- As the blood flow to the atria increases, atrial Natriuretic Factor (ANF) is released.
- ANF causes vasodilation and decreases blood pressure. It checks renin-angiotensin mechanism.
Micturition
- The stretch receptors on the walls of the urinary bladder send signals to the CNS whenever it gets filled with urine, the CNS passes motor messages to initiate the contraction of smooth muscles and relaxation of the urethral sphincter causing the micturition.
- The urine formed is light yellow coloured fluid with pH-6.0. On an average , 25-30 gm of urea is excreted per day.
- Presence of glucose (glycosuria) and ketone bodies (ketonuria) in urine are indicative of dia-betes mellitus.
- Urine that is excreted out consists of 90% water, 2% Urea & 2% of other dissolved solutes
Role of Other Organs In Excretion
- Lungs remove large amounts of CO2 (18 litres per day) and H2O .
- Liver secretes bilirubin, biliverdin, cholesterol, degraded steroid hormones, vitamins and drugs, they pass out along with digestive wastes.
- Sweat glands remove NaCl, urea , lactic acid, etc.,
- Sebaceous glands eliminate sterols, hydrocarbons and waxes.
- Small amounts of nitrogenous wastes are also eliminated through saliva.
8. DISORDERS OF THE EXCRETORY SYSTEM Uremia
- Accumulation of urea in blood is called uremia and that urea can be removed by a process called haemodialysis.
- Kidney transplantation is the ultimate method in the correction of acute renal failures.
Renal calculi
- Renal calculi are stones or insoluble masses of crystallised salts like oxalates, uricacid etc formed with in the kidney.
Glomerulonephritis
- Inflammation of glomeruli of kidney.
Renal failure
- Renal failure is typically detected by an elevated serum creatinine level.
Artificial kidney
- Artificial kidney /dialyser, is a machine that is used to filter the blood of a person whose kidneys are damaged, this process is called hemodialysis.
- The dialyzing fluid has the same composition as that of plasma , except the nitrogenous wastes.
- In this process blood is taken out from the main artery mixed with an anticoagulantheparin, and then pumped into the dialyser. The cleared blood is pumped back to the body through a vein after adding anti-heparin to it.
- Each dialysis session lasts 2-6 hours.
Renal abnormalities
| Abnormalities | Description |
| 1 Albuminuria | Presence of albumin in urine |
| 2 Bright’s disease | Inflammation of kidney (=Glomerulonephritis) |
| 3 Cystitis | Inflammation of lining of the urinary bladder |
| 4 Diabetic Nephropathy | A disease of the kidney associated with diabetes mellitus; it is the principal cause of chronic renal failure |
| 5 Diuretics | Chemicals that increase urine volume |
| 6 Dysuria | Painful urination |
| 7 Enuresis | Bed-wetting |
| 8 Glycosuria | Presence of glucose in urine. A pathological glycosuria results from diabetes mellitus |
| 9 Gout | High level of uric acid in the blood |
| 10 Haematuria | Presence of blood (RBCs) in urine |
| 11 Haemoglobinuria | Presence of haemoglobin in urine |
| 12 Ketonuria | Presence of ketone or acetone bodies (acetoacetic acid, -hydroxybutyric acid and acetone) in urine(=Acetonuria)Ltd., |
| 13 Polycystic kidney | A genetic disease due to an autosomal dominant mutation of a gene located on chromosome 16 |
| 14 Polyuria(=diuresis) | An output in excess of urine 20 litres/day India |
| 15 Proteinuria | Excess protein in urine |
| 16 Shock-wave lithotripsy diaMultim | A technique to remove kidney stones with ultrasound or lasers· |
| 17 Uraemia | High blood urea level due to kidney failure |
ADDITIONAL POINTS
- Based on the maintenance of water animals are Osmoconformers – to be isotonic with their surroundings, all are marine.eg: Most marine invertebrates, some marine vertebrates like hag fish etc., Osmoregulators – to control internal osmolarity independent of that of its environment. eg: Most vertebrates except hag fish and elasmobranchs.
- Organisms which cannot tolerate substantial changes in external osmolarity are said to be stenohaline, whereas animals that can survive large fluctuations in external osmolarity are euryhaline. Eg: Salmon and Eel.
- Freshwater animals face the problem of gaining water by osmosis and losing salts by diffusion. In protozoans contractile vacuoles pump out excess water, ionocytes or chloride cells in the gill membrane of freshwater fish can actively transport Cl– into the body and allow Na+ .
- In marine bony fishes ionocytes or chloride cells actively transport Cl– out and allow Na+ . In sea turtles and birds salt glands excrete excess salts. Elasmobranchs and Coelacanths retain urea and
- Euryhaline fishes while living in freshwater they produce large amounts of dilute urine, when they migrate to the ocean they drink sea water and produce only small amounts of urine.
- Humans die if they lose around 12 % of the body water. Kangaroo rats can recover 90% of the loss by using metabolic water and 10% from its diet of seeds.
- Camels can live even after losing about 20% of the body water .They produce dry faeces and concentrated urine. When water is not available, they do not produce urine but store urea in tissues and solely depend on metabolic water derived from catabolism of fat stored in the hump.
- Nephrology is the study of the anatomy, physiology and pathology of the kidneys.
- The branch of medicine that deals with the male and female excretory systems and the male reproductive system is called urology.
- Kidneys are partially protected by the eleventh and twelfth pairs of ribs.
- Three layers of tissue surround each kidney are renal capsule, perirenal fat and renal fascia from inner to outer.